안녕하세요! 헬씨부입니다~

오늘은 ' 항응고제 - 와파린 [ Warfarin ], 헤파린 [heparin] '에 대해 알아보고 정리하겠습니다!
항응고제
와파린 [ Warfarin ], 헤파린 [heparin]

정의
항응고제(anticoagulant)는 혈액 응고를 방지하거나 감소시켜 응고 시간을 연장시키는 화학 물질이다. 항응고제 중 일부는 거머리나 모기와 같은 흡혈동물들에서 자연적으로 생성되며, 물린 부위가 흡혈 동물이 피를 얻을 수 있을 만큼 충분히 응고되지 않도록 유지하는 데 도움을 준다. 의약품의 한 종류로서의 항응고제는 혈전증 치료에 사용됩니다
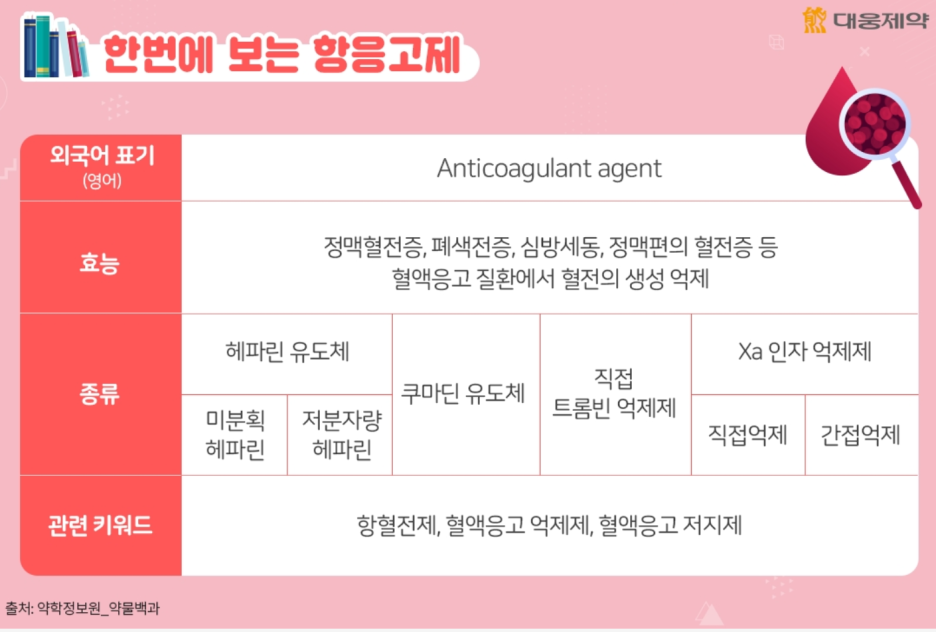
항응고제는 혈액의 응고 능력을 감소시키는 원리로 혈관 내에 비정상적으로 일어나는 혈전 형성을 방지하는 약물입니다. 주로 정맥혈전증이나 폐색전증, 심장판막 수술, 심방세동, 뇌경색 등 혈액응고 질환의 예방과 치료에 사용됩니다.
단, 항응고제의 부작용으로 출혈 위험이 증가할 수 있습니다. 따라서 중대한 출혈이 발생할 경우 투여를 멈추고 신속히 의료기관에 방문해야 합니다.

작동원리

항응고제의 작용 원리를 살펴보기 전, 혈전(혈관 속에서 혈액이 굳어진 덩어리)의 생성 과정을 알아보겠습니다. 혈관에 손상이 생기면 혈구 세포 중 하나인 혈소판이 손상 부위에 붙어 덩어리를 만들게 됩니다. 그 후, 혈액 응고 단백질들이 섬유소 망을 단단히 뭉치게 만들어 혈액을 응고시키면서 혈전이 생성됩니다.
항응고제는 혈전 생성의 두 번째 단계인 혈액응고 과정을 억제해, 혈전 생성을 막습니다.
항응고제 종류

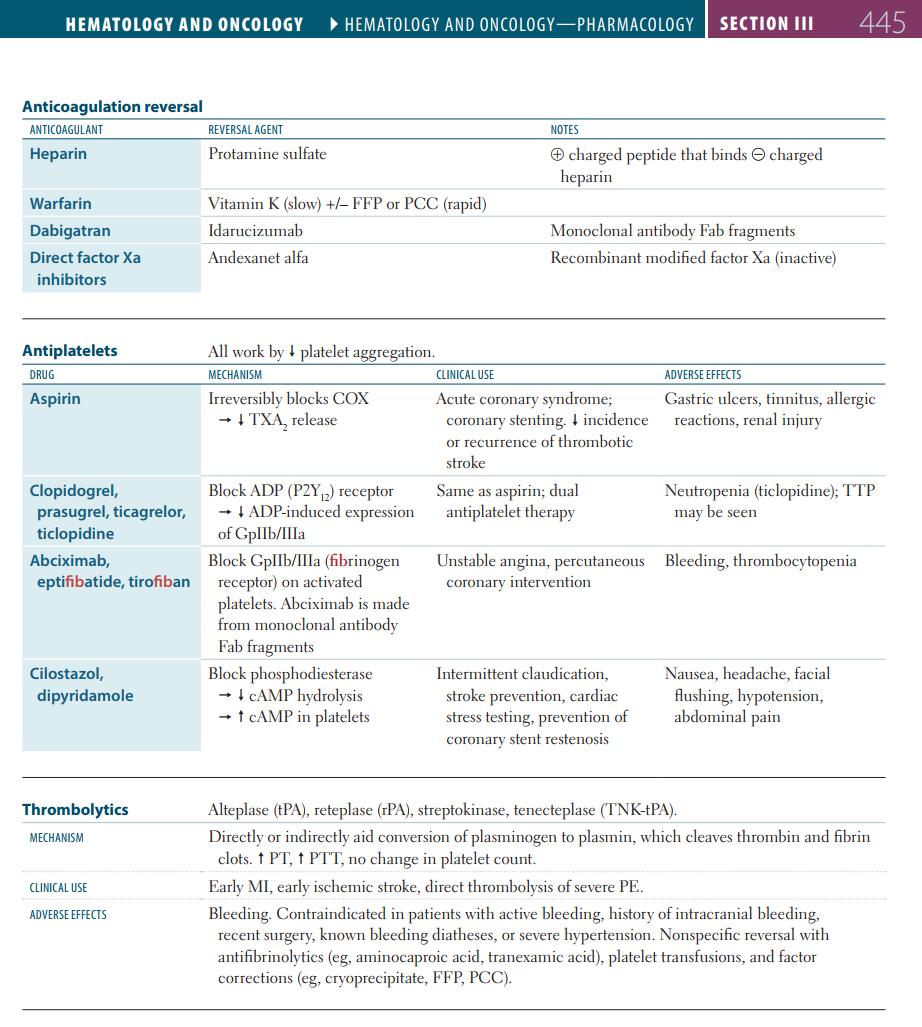
항응고제는 작용 원리에 따라 헤파린 유도체, 쿠마딘 유도체, 직접 트롬빈 억제제, Xa 인자 억제제로 구분할 수 있습니다.
헤파린 유도체는 미분획 헤파린이라고도 하는데, 혈액 응고를 방지하지만 출혈을 일으킬 수 있고 개인에 따라 항응고 효과의 정도가 다양하게 나타나므로 주기적으로 aPTT 검사를 통해 용량을 조절해야 합니다. 저분자량 헤파린은 헤파린의 단점을 개선하기 위해 헤파린을 화학적, 물리적으로 분해한 것인데요. 용량에 따른 항응고 효과에 대한 예측이 가능해 혈액응고 검사를 할 필요가 없으며 투여방법이 간편하고 부작용이 적은 편입니다. 그러나 신부전 환자는 용량을 조절해야 합니다.
쿠마딘 유도체는 비타민K의 작용을 차단해 비타민K를 필요로 하는 응고인자의 활성화를 억제하는데요. 복용이 편하고 가격도 저렴하지만 작용 발현이 늦게 나타나고 혈액 응고 검사를 통해 용량을 조절해야 합니다.
직접 트롬빈 억제제는 트롬빈에 직접 부착해 작용을 차단하는 약물입니다.
Xa 인자 억제제는 혈액응고 단계에서 Xa 응고인자를 선택적으로 저해해 혈전의 생성을 막는데요. 경구투여로 복용이 편하고, 와파린의 출혈 부작용이나 약물상호작용, 음식 상호작용이 적습니다.
항응고제 주의사항
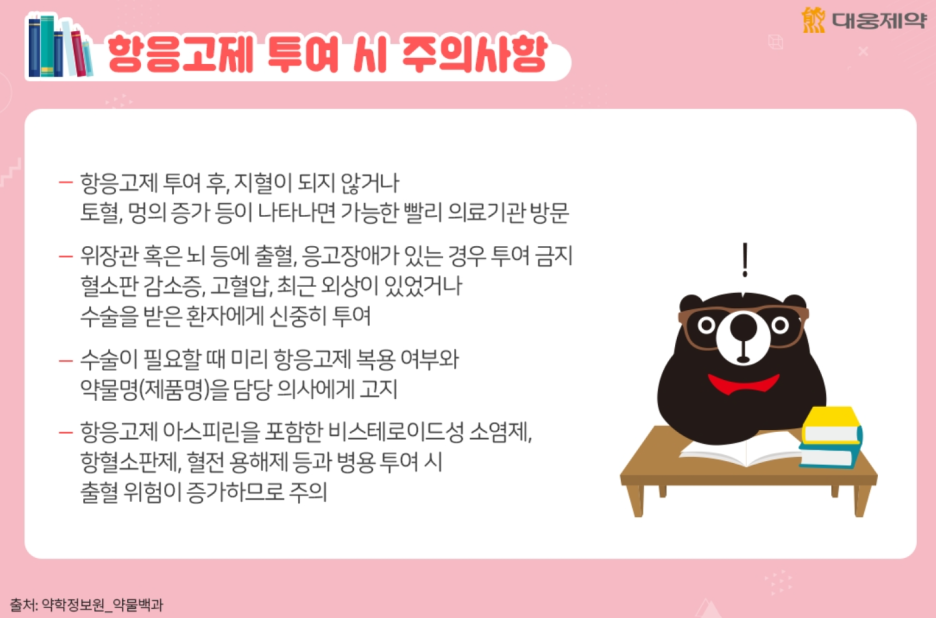
항응고제 투여시 잇몸 출혈, 피부의 멍, 코피 등이 나타날 수 있는데요. 지혈이 되지 않거나 토혈, 혈뇨, 멍의 증가, 과다출혈 등의 경우 응급상황일 수 있어 가능한 빨리 의료기관을 방문해 의료진과 상의해야 합니다.
항응고제는 위장관 혹은 뇌 등에 출혈이 있거나, 응고 장애가 있는 환자에게 투여가 금지됩니다. 또, 혈소판 감소증, 고혈압, 최근 외상이 있었거나 수술을 받은 환자에게도 신중히 투여할 필요가 있고요.
평소 항응고제를 투여하는 환자가 부득이하게 수술을 받아야 한다면 미리 항응고제의 복용 사실과 약물명을 담당 의사에게 알려야 합니다.
그외 자세한 사항은제품별 설명서 또는 허가정보에서 확인할 수 있습니다.
문제
A 62-year-old man, who is known to have recurrent thromboembolic strokes, presents to his physician for a routine follow-up visit. While assessing drug compliance, the physician realizes that the patient inadvertently doubled his dose of warfarin 1 month ago. When he is asked about any new complaints, the patient denies any symptoms, including bleeding. The physical examination does not show any signs of bleeding. Based on the patient’s lifestyle, the physician does not consider him to be at increased risk for bleeding. He then orders international normalized ratio (INR) testing for this patient, which yields a value of 13. In addition to temporarily withholding warfarin, which of the following drugs is indicated for this patient?
|
|
Explanation:
Correct answer B: When patients present with an overdose of warfarin, the pertinent factors that guide treatment include the presence of active bleeding and the INR level. This patient does not have any signs of active bleeding, but his INR is very high (> 10), so the treatment would be to temporarily withhold warfarin and give a dose of oral phytonadione (vitamin K1). The INR would then be followed closely and the correct dose of warfarin would be restarted once the INR returns to the goal range (which usually takes several days). Patients with an INR is 4.5—10 and no bleeding are treated similarly, however the oral vitamin K is somewhat optional (many physicians still opt to give vitamin K in this scenario, given the high risk of bleeding at these elevated INR levels). Patients that have an INR < 4.5 and no bleeding are managed by withholding warfarin and monitoring the INR closely, but do not need to be administered vitamin K. Patients that have serious bleeding at any level of supratherapeutic INR (which is usually any level above 3) will need intravenous vitamin K, along with prothrombin complex concentrate (PCC). Fresh frozen plasma (FFP) can be also be used instead of PCC, however PCC is preferred. It is important to remember that vitamin K1 re-establishes the activity of clotting factors and does not affect the plasma levels of warfarin. Response to vitamin K1 takes approximately 24 hours to bring about a reduction in INR; therefore, PCC or FFP is necessary when immediate hemostasis is required (PCC reduces the INR within 1 hour). Warfarin is a widely used coumarin anticoagulant that blocks the γ-carboxylation of glutamate residues in factors II, VII, IX, and X. Warfarin also inhibits proteins C and S. Vitamin K plays an essential role in the carboxylation and reactivation of these factors and is used an antidote for warfarin overdose/toxicity. Vitamin K1 (phytonadione) is commercially available in oral and parenteral forms, while vitamin K2 (menaquinone) is synthesized by intestinal bacterial flora and is naturally present in human tissues. Option A: Although the patient is not bleeding, the INR is too high (>10) to simply withhold a dose of warfarin. In this situation (i.e. INR >10, but no bleeding), some physicians might only hold the warfarin, but not give oral vitamin K, however they would check the INR repeatedly (over the course of several days), and wait until it fell into the goal range before resuming warfarin at the correct dose. Option D: Menaquinone (vitamin K2) is the natural form of vitamin K. Menaquinone is synthesized by the human intestinal bacteria and is not available commercially. Option C: Recombinant Factor VIIa (rFVIIa) is a synthesized clotting factor used for perioperative prophylaxis in patients with hemophilia. Factor VII is not commonly used for the reversal of supratherapeutic INR from warfarin overdose. Option E: Protamine sulfate is an antidote for bleeding caused by heparin. It is not used for warfarin toxicity. Option F: Tranexamic acid is an antidote for bleeding caused by fibrinolytic states. It is not used for warfarin toxicity. Learning objective: Vitamin K acts as an antidote for warfarin toxicity because it plays an essential role in the carboxylation and reactivation of the vitamin K-dependent clotting factors (II, VII, IX, X and proteins C and S). The response to vitamin K1 (phytonadione) takes approximately 24 hours to reduce the INR. Therefore, prothrombin complex concentrate (PCC) or fresh frozen plasma (FFP) is also indicated when immediate hemostasis is required in actively bleeding patients. |
|
Related Videos:
|
|
Book References:
First Aid for the USMLE Step 1 (2022, 32nd ed): 69, 445, 444 First Aid for the USMLE Step 1 (2021, 31st ed): 71, 446, 447 First Aid for the USMLE Step 1 (2020, 30th ed): 71, 413, 436 First Aid for the USMLE Step 1 (2019, 29th ed): 71, 405, 428 First Aid for the USMLE Step 1 (2018, 28th ed): 71, 402, 424 First Aid for the USMLE Step 1 (2017, 27th ed): 66, 392, 414 |
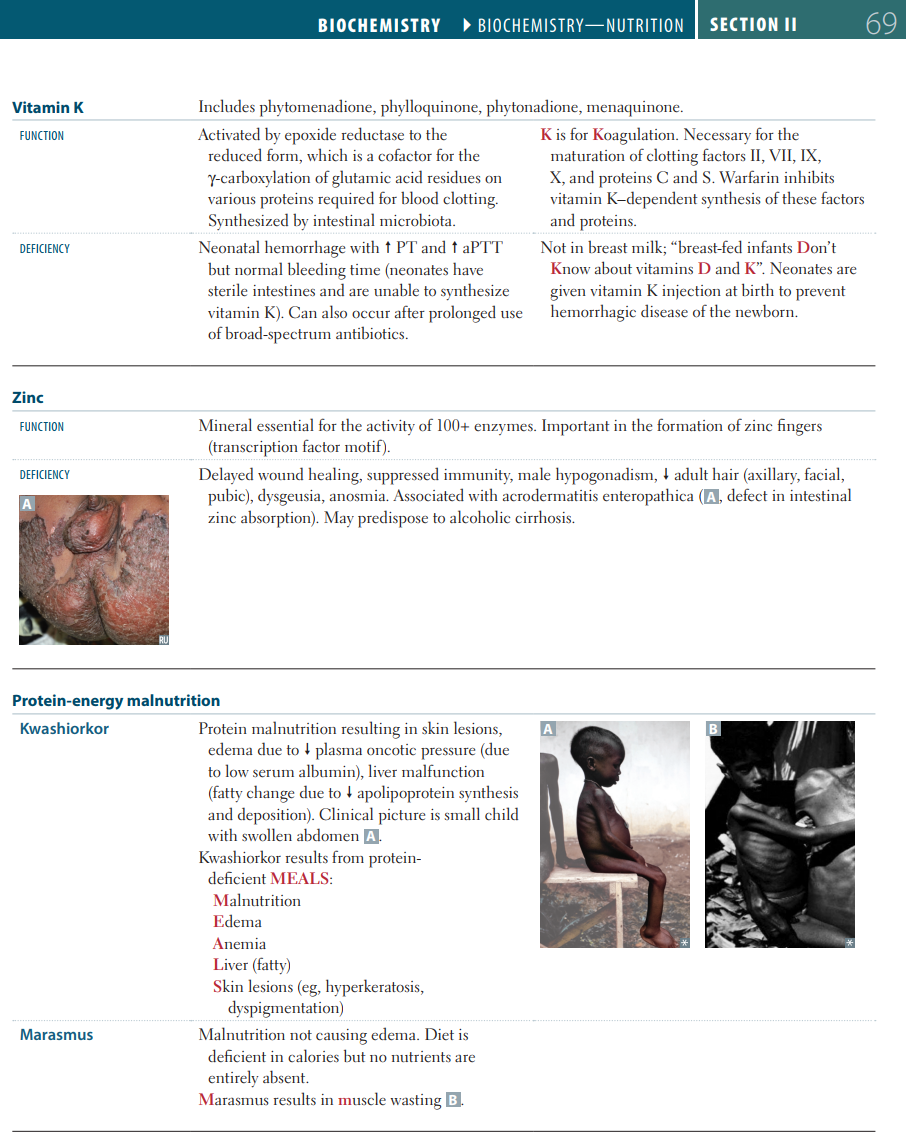
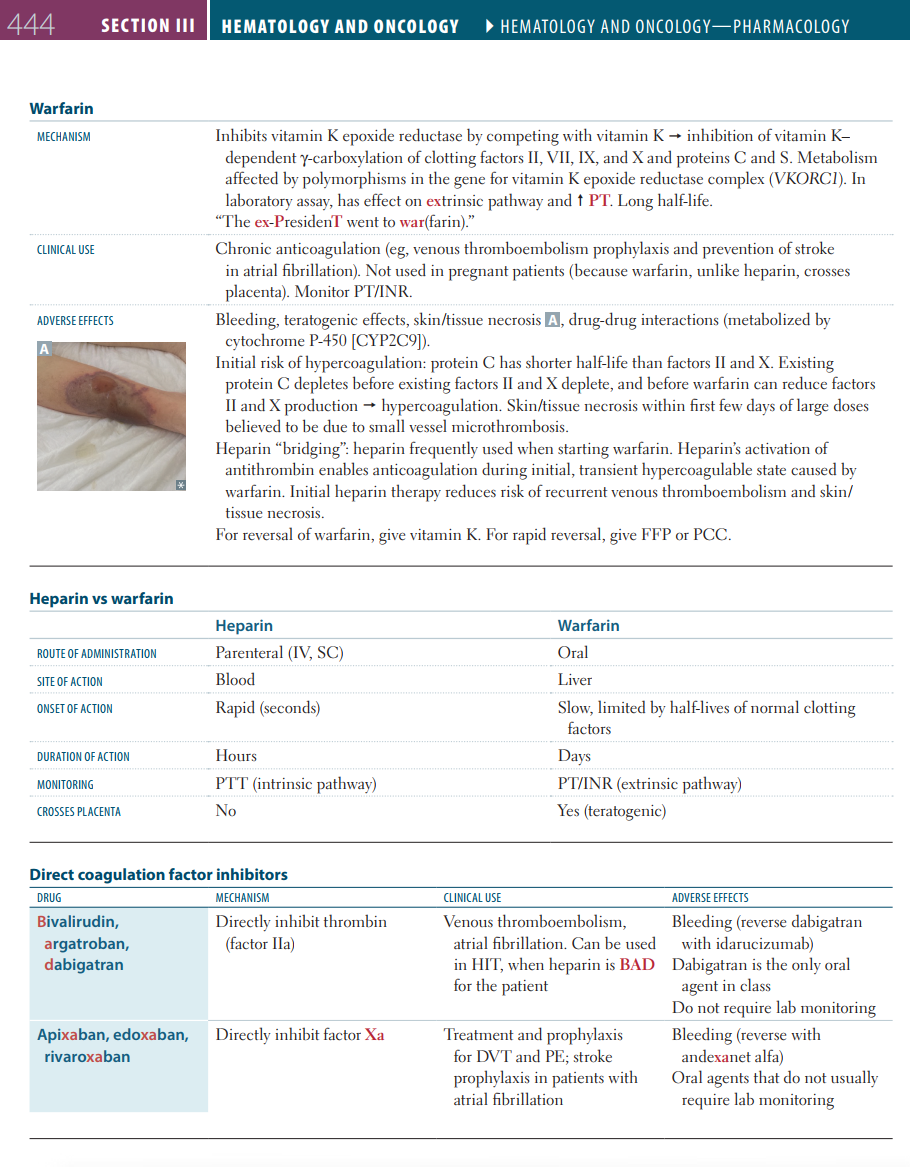
사진 설명을 입력하세요.
참고자료
오늘은 여기까지 정리하겠습니다!
감사합니다!

댓글